
Child and Adolescent Psychiatry Policy Manual
Preface—Our Vision and Mission
The Scope of This Manual
Message from the Program Director
Message from the Associate Program Director
Aims of the Child and Adolescent Psychiatry Program
General Information for Faculty Members
ACGME Common Program Requirements
Faculty Responsibilities
Faculty Development
Faculty Qualifications
ACGME Specialty Review Committees
Graduate Medical Education Personnel
Current Core and Adjunct Faculty
Child and Adolescent Psychiatry Fellow Roster
Orientation and Child Psychiatry Bootcamp
Child and Adolescent Psychiatry Fellow Benefits
General Information
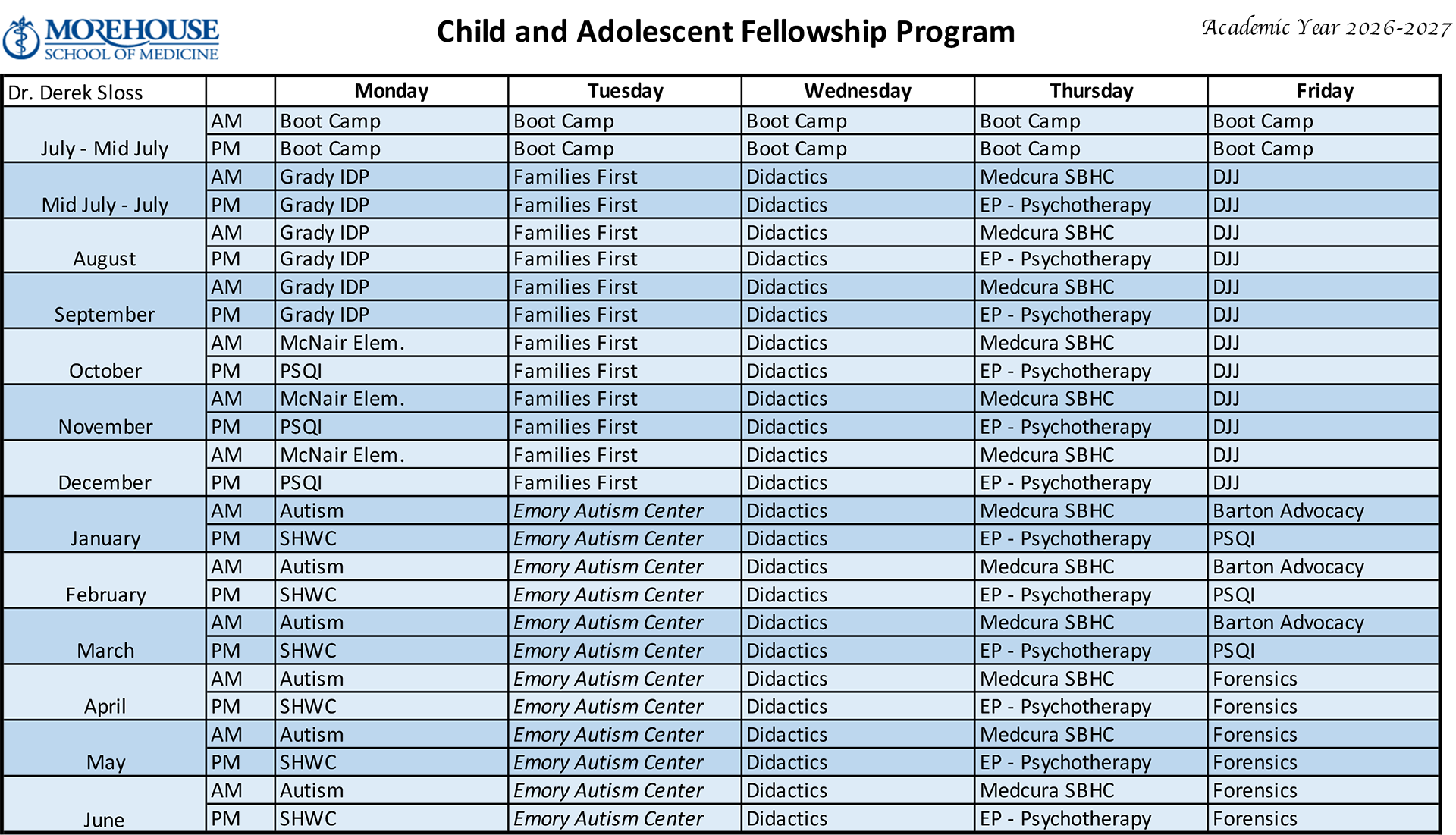
CAP Fellowship Master Clinical Schedules
Learning Activities
Educational Program Requirements
Child and Adolescent Psychiatry Fellow Position Summaries
Goals, Objectives, Key Personnel, and Site Information by Rotation
Policies, Procedures, Processes, and Program Templates
ACGME Program Requirements for Graduate Medical Education in Child and Adolescent
Psychiatry
Preface—Our Vision and Mission
MSM Vision
Leading the creation and advancement of health equity by:
- Translating discovery into health equity
- Building bridges between health care and health
- Preparing future health learners and leaders
MSM Mission
We exist to:
- Improve the health and well-being of individuals and communities;
- Increase the diversity of the health professional and scientific workforce
- Address primary health care needs through programs in education, research, and service, with emphasis on people of color and the underserved urban and rural populations in Georgia, the nation, and the world.
Morehouse School of Medicine (MSM) is like no other medical school in the country. Like other schools, we attract students who want to be great doctors, scientists, and health care professionals, and who want to make a lasting difference in their communities. However, MSM ranks number one in the first-ever study of all United States medical schools in the area of social mission.
The ranking came as a result of MSM’s focus on primary care and its mission to address the needs of underserved communities, a commitment which the study emphasizes is critical to improving overall health care in the United States. Such recognition underscores the vital role that MSM and other historically black academic health centers play in the nation’s health care system by addressing, head on, the issues of diversity, access, and misdistribution.
Put simply, we attract and train the doctors and health professionals America needs most: those who will care for underserved communities; those who will contribute racial and ethnic diversity to the health professions and scientific workforce; those who will dedicate themselves to eliminating the racial, ethnic, and geographic health inequities that continue to plague the community and the nation.
Likewise, our researchers seek to understand not only the biological determinants of illness and health, but also the social determinants: the circumstances in which someone is born, lives, works, and ages. These circumstances can be shaped by diverse forces, but can be just as powerful as physiology, if not more so, when it comes to health and wellness.
The Scope of This Manual
The Child and Adolescent Psychiatry (CAP) Policy Manual is an outline of the basic CAP policies, practices, and procedures at Morehouse School of Medicine (MSM or School). The Child and Adolescent Psychiatry Policy Manual is intended only as an advisory guide. The term resident in this document refers to both specialty residents and subspecialty fellows.
This policy manual should not be construed as, and does not constitute, an offer of employment for any specific duration. This policy manual does not constitute an expressed or implied contract of employment for any period of time. Either MSM or an employee may terminate the employment relationship at any time with or without cause and with or without notice.
MSM will attempt to keep the Child and Adolescent Psychiatry Policy Manual and its online version current, but there may be cases when a policy will change before this material can be revised online. Therefore, you are strongly urged to contact the Child and Adolescent Psychiatry Office to ensure that you have the latest version of MSM’s policies.
Policy updates will be communicated to the MSM community via email and will be posted on the MSM internet site. MSM may add, revoke, suspend, or modify the policies as necessary at its sole discretion and without prior notice to employees. This right extends to both published and unpublished policies. A copy of the Child and Adolescent Psychiatry Policy Manual is available for download from the MSM website.
The current MSM Policy Manual supersedes all previous Child and Adolescent Psychiatry Policy Manuals, policies, and employee handbooks of MSM. The effective date of each policy indicates the current policy and practice in effect for the school.
Message from the Program Director

Greetings!
The Morehouse School of Medicine Child Psychiatry Program is excited to partner with you on your journey to become a child and adolescent psychiatrist. We are honored that you trusted us with your training and are committed to, and intentional about, our goal: developing excellent clinicians and effective advocates primed to make an impact in our communities.
This program is designed to provide you with a diversity of scholarly and clinical activities that increase your professional skills, medical knowledge, and clinical acumen. Just as importantly, it includes learning opportunities that will equip you to leverage your privilege, knowledge, and power to work collaboratively and innovatively across disciplines to advance children’s mental health. To this end, the program provides you a broad-based training experience achieved through partnership with a variety of agencies: community- and academia-based organizations; private and public mental health care providers; and educational and legal institutions.
While rewarding, the work of child and adolescent psychiatry is challenging, nuanced, and demanding. As you learn to navigate patient care, self-care, professional development, and worklife integration in this new role, our faculty aims not only to provide guidance as it relates to the nuts and bolts of psychiatric practice, but also to serve as mentors and sources of support. They, along with the Morehouse School of Medicine administration and staff, value you and your wellness.
Mental health matters for every aspect of society. Healthy growth and development, and children’s mental health promotion are critical in the creation and advancement of health equity. Thank you for joining us in this work. And welcome!

Danae Evans, M.D.
Program Director of the Child and Adolescent Psychiatry Fellowship Program
Message from the Associate Program Director

I bring you greetings from Morehouse School of Medicine Child and Adolescent Psychiatry Fellowship Program leadership!
It is with great pleasure that I welcome you to train at our very special community-based program. As the program enters its third academic year, we are happy to announce that we have achieved continued accreditation and that we graduated our inaugural class in 2022! In fact, we have already seen new heights and expansion.
With over 20 community sites, your educational learning experience at Morehouse School of Medicine will encompass a variety of clinical settings, from inpatient psychiatric hospitals to consultation-liaison, to community mental health agencies, to school-based mental health clinics, not to mention the plethora of specialty electives we offer. This range of opportunities gives our program the unique benefit of being a true community-based program.
As is inherent in our vision and mission, we strive to pave the way for the education and advancement of young mental health professionals who will, in turn, provide the utmost care to historically marginalized and disadvantaged communities. We aim to diversify the health care workforce while increasing access to mental health care for those in greatest need.
It is an honor to be your Associate Program Director. I thoroughly enjoy working with our fellows and look forward to participating in your training through multiple levels of didactics, mentorship, and beyond. Please do not hesitate to email, text, or call me with questions and concerns. We are a team here at Morehouse School of Medicine and are here to support you through your journey to the next level in your awesome career!
Again, Welcome!
Kamille Williams, M.D.
CAP Fellowship Faculty
Associate Program Director of the Child and Adolescent Psychiatry Fellowship Program
Morehouse School of Medcine
Aims of the Child and Adolescent Psychiatry Program
The Child and Adolescent Psychiatry Program has three primary aims:
- Provide a training experience that inspires child and adolescent psychiatry fellows to provide quality health care to all, especially historically marginalized and under-resourced populations in Georgia;
- Promote scholarship and leadership in the fields of child psychiatry by our faculty and fellows, by supporting advocacy, alliance-building, and academic pursuits;
- Deliver an academically rigorous, clinically relevant, and culturally and structurally informed training experience for our fellows that equips them to be excellent clinicians and effective physician advocates.
General Information for Faculty Members
The Graduate Medical Education Committee (GMEC) highly values the contributions of our faculty members. The GMEC agrees with, supports, and adheres to the ACGME requirements and standards as related to faculty members reflected in the following section of the ACGME Program Requirements for Graduate Medical Education in Child and Adolescent Psychiatry, Common Program Requirements from July 1, 2025:
Faculty members are a foundational element of graduate medical education—faculty members teach fellows how to care for patients. Faculty members provide an important bridge allowing fellows to grow and become practice ready, ensuring that patients receive the highest quality of care. They are role models for future generations of physicians by demonstrating compassion, commitment to excellence in teaching and patient care, professionalism, and a dedication to lifelong learning. Faculty members experience the pride and joy of fostering the growth and development of future colleagues. The care they provide is enhanced by the opportunity to teach. By employing a scholarly approach to patient care, faculty members, through the graduate medical education system, improve the health of the individual and the population.
Faculty members ensure that patients receive the level of care expected from a specialist in the field. They recognize and respond to the needs of the patients, fellows, community, and institution. Faculty members provide appropriate levels of supervision to promote patient safety. Faculty members create an effective learning environment by acting in a professional manner and attending to the wellbeing of the fellows and themselves.
ACGME Common Program Requirements
For each participating site, there must be a sufficient number of faculty members with competence to instruct and supervise all fellows at that location.
Faculty members must:
- Be role models of professionalism;
- Demonstrate commitment to the delivery of safe, quality, cost-effective, patient-centered care;
- Demonstrate a strong interest in the education of fellows;
- Devote sufficient time to the educational program to fulfil their supervisory and teaching responsibilities;
- Administer and maintain an educational environment conducive to educating fellows;
- Regularly participate in organized clinical discussions, rounds, journal clubs, and conferences; and
- Pursue faculty development designed to enhance their skills at least annually:
Faculty Development is intended to describe structured programming developed for the purpose of enhancing transference of knowledge, skill, and behavior from the educator to the learner. Faculty development may occur in a variety of configurations (lecture, workshop, etc.) using internal and/or external resources. Programming is typically needs-based (individual or group) and may be specific to the institution or the program. Faculty development programming is to be reported for the fellowship program faculty in the aggregate.
Faculty members must:
- Have appropriate qualifications in their field and hold appropriate institutional appointments;
- Subspecialty physician faculty members must have current certification in the subspeciality by the American Board of Psychiatry and Neurology or the American Osteopathic Board of Neurology and Psychiatry, or possess qualifications judged acceptable to the Review Committee.
Any non-physician faculty members who participate in fellowship program education must be approved by the program director.
Core faculty members must:
- Have a significant role in the education and supervision of fellows;
- Devote a significant portion of their entire effort to fellow education and/or administration;
- Teach, evaluate, and provide formative feedback to fellows as a component of their activities; and
- Complete the annual ACGME Faculty Survey.
ACGME Specialty Review Committees
ACGME Specialty Review Committees:
- May further specify additional physician and non-physician faculty member qualifications;
- Must specify the minimum number of core faculty and/or the core faculty-to-fellow
ratio;
and - May specify requirements specific to associate program director(s).
Graduate Medical Education Personnel
| Senior Associate Dean/ Designated Institutional Official |
Associate Dean Graduate Medical Education |
Executive Director Graduate Medical Education |
| Chinedu Ivonye, MD, FACP civonye@msm.edu |
Riba Kelsey, MD, FAAFP rkelsey@msm.edu |
Susan Ratliff, MBA, C-TAGME sratliff@msm.edu |
| Graduate Medical Education Associate Director |
Institutional Program Manager |
Data Management Specialist |
| Tiffany Burns tburns@msm.edu |
Yvonne Gilbert, MPH, C-TAGME ygilbert@msm.edu |
Felicia Underwood funderwood@msm.edu |
| GME Assistant to the Designated Institutional Official |
Fellowship Program Manager | Fellowship Program Coordinator |
| Yvonne Jones yvojones@msm.edu |
Kennyna Landing, BS klanding@msm.edu |
Kristopher Goodlow krgoodlow@msm.edu |
Current Core and Adjunct Faculty
| Core Faculty |
| Department Chair Sarah Y. Vinson, MD svinson@msm.edu |
Program Director Danae Evans, MD danevans@msm.edu |
Associate Program Director Kamille Williams, MD kwilliams@msm.edu |
| Vice Chair Nicole Cotton, MD ncotton@msm.edu |
Core Faculty Shaakira Ford, LCSW, DSW saford@msm.edu |
Core Faculty Jenika Hardeman, PhD jhardeman@msm.edu |
| Core Faculty Leroy Reese, PhD lreese@msm.edu |
Core Faculty Marietta Collins, PhD mcolllins@msm.edu |
|
| Additional CAP Faculty |
| Ranjan Avasthi, MD RAVASTHI@augusta.edu |
Hasani Baharanyi, MD drbaharanyi@hakiwellness.com |
Anastasia Brown-Alvarado, MD Anastasia.Alvarado@choa |
| Melissa Carter, JD melissa.d.carter@emory.edu |
Beverly Stoute, MD beverlystoutemd@gmail.com |
Yolanda Fountain, PhD drfountain@playwellness.net |
| Ayo Gathing, MD ayoa23@hotmail.com |
Kenneth Genova, MD kgenova@tanner.org |
Ericka Goodwin, MD, DFAPA kiddieshrink@mac.com |
| Marcus C. Griffith, MD marcus.c.griffith@kp.org |
Jamila Hallman-Cooper, MD hallmancooper@emory.edu |
Steven L. Jaffe, MD srjaffe@bellsouth.net |
| Sherri Simpson-Braodwater, MD sherri_simpson@hotmail.com |
Jonathan Levy, MD jonathan.levy@emilyprogram.com |
Sarah Herbert, MD saraheherbertmd@gmail.com |
| Bret Murphy-Dawson, MD bmurphydawson@msm.edu |
Kristin Weinschenk, MD Kristin.weinschenk@choa.org |
Theodore Morgan, MD thmorgan2@mymindsbeauty.com |
| Fatima Kasiah, MD fkasiah@msm.edu |
Sheritta Carmichael, MD scarmichael@msm.edu |
Gail Mattox, MD gmattox@msm.edu |
Child and Adolescent Psychiatry 2026-2027 Fellow Roster
First Year Fellows



Second Year Fellows

Orientation and Child Psychiatry Bootcamp
GME and institutional orientation for new fellows is held during the first several weeks of their F-1 year. Orientation includes information about the GME office, institution, policies, evaluation procedures, and benefits.
During their program-specific orientation, fellows receive an introduction to the administrative and academic requirements of the Child and Adolescent Psychiatry Fellowship Program and the Department of Psychiatry. They are provided information about the faculty, rotation schedules, conferences, advisors, and clinical and didactic learning activities.
Throughout the two years of fellowship training, the following records will be retained in each fellow’s permanent file:
- ERAS application and supplemental materials
- Credentials, including degree, transcripts, and curriculum vitae
- Copies of temporary training permits, licensure, liability insurance
- Transfer records indicating previous training, performance, and a statement of integrity
- Examination scores (USMLE, Clinical Competency Exam, In-Training Exam)
- Signed attestation indicating receipt of goals and objectives
- Evaluation summaries
- Evidence of scholarly and PS/QI activity
- Patient logs
- Due process and grievance proceedings (when applicable)
- Checklist and verification statements from the program director, upon completion of the program
- Annual Training Agreement
The fellow’s file is the property of the Morehouse School of Medicine CAP Fellowship Department.
Child and Adolescent Psychiatry Fellow Benefits
The following benefits are offered to Child and Adolescent Psychiatry fellows:
- Medical and dental insurance
- Life insurance
- Professional liability insurance
- Sick leave (15 days/year)
- Vacation (15 days/year)
- White coats (2)
- Administrative/educational leave (The 10-day baseline may be modestly increased for fellows participating in national meetings, boards, or committees, at the program director’s discretion)
General Information
Adherence to Policies and Procedures
All fellows must comply with the policies and procedures of the program, GME, MSM, and all affiliate hospitals and sites where rotations are provided. The electronic version of this manual can be found on the Child and Adolescent Psychiatry Fellowship home page in MedHub.
NOTE: You must respond to a call at all times while on duty.
Paychecks
Paychecks are available per the institutional pay schedule.
Licensure Policy
Fellows are required to apply for and have their full Georgia State Medical License and Drug Enforcement Administration License prior to entrance to the program. This is paid for by the institutional GME or fellowship as reimbursement. Fellows should obtain licensure once the official match season has ended along with receiving confirmation and contract from the Fellowship. Fellows can apply through the licensure link:
https://medicalboard.georgia.gov/licensure-information/physician and https://www.deadiversion.usdoj.gov/online_forms_apps.html.
Certifications
Fellows are required to be certified and maintain certification in Advanced Cardiac Life Support (ACLS) and Basic Life Support (BLS) throughout their fellowship.
NPI Number
If a fellow has not applied for a NPI and he/she/they has a Social Security Number, the fellow must complete the online application at https://nppes.cms.hhs.gov/#/.
If a fellow has not applied for an NPI and he/she/they does not have a Social Security
Number, the fellow must complete the paper application found at the following link:
http://www.cms.gov/Medicare/CMS-Forms/CMS-Forms/Downloads/CMS10114.pdf.
If a fellow is coming to a Morehouse School of Medicine-sponsored program and already has an NPI, the fellow must change the business address of the previous NPI number to their new program’s mailing address. The fellow can get information by contacting the program.
Fellows must use their NPI number for writing prescriptions.
Mailboxes
Fellow mailboxes are located in the Department of Psychiatry in the Hurt Building. Fellows should purge their mailboxes on a weekly basis. We strongly encourage fellows to make an effort to change all mailing addresses to their home address; doing so ensures that fellows receive important mailings in a timely fashion.
Professional Organizations
The program provides support for the fellow’s annual membership in the American Academy of Child and Adolescent Psychiatry (AACAP). We strongly recommend that each fellow becomes an active member of the Georgia Chapter of AACAP and takes full advantage of the organization’s educational resources. Additionally, we encourage fellows to consider participation in the American Association of Community Psychiatry, the American Academy of Pediatrics, the Black Psychiatrists of America, and the American Psychiatric Association.
Administrative/Educational Leave
The program provides fellows a maximum of 10 days paid administrative leave to attend educational-based conferences. This time away applies to the entire two (2) years of fellowship training and is based on prior approval from the program director. Leave for job interviews for second year fellows should be scheduled on the fellow’s day off. Additional time off for interviews will be decided on a case-by-case basis. All leave must be approved by the program director.
Faculty Advisor Roles and Responsibilities
At the beginning of each academic year, MSM Child and Adolescent Psychiatry faculty members are selected to serve as faculty advisors for incoming fellows. Those faculty members selected each serve as an advisor/coach for a selected fellow for the entire two (2) years of their fellowship.
Faculty advisors serve as a resource, a coach, a role model, and a teacher. Although the role of advisor is multi-faceted, and the day-to-day responsibilities vary depending on the fellow, an outline of the basic roles and responsibilities of the faculty advisor are listed below.
The following qualifications and responsibilities apply to faculty advisors:
- Be dedicated and enthusiastic about the fellow’s education.
- Challenge and encourage fellows to be exemplary in their profession
- Serve as role models for patient interactions.
- Encourage positive interaction and problem-solving skills
- Advise the fellow on timely fulfillment of requirements (scholarly activity, duty hours, patient logs, etc.), improving study habits, and issues related to professionalism.
- Ensure that fellows are preparing themselves for life beyond fellowship to include guidance in the process of applying for exploration of other professional pursuits (private practice, academic medicine, etc.).
- Act as a liaison between the individual fellow and the administration.
- Provide the fellow opportunities to discuss confidential issues.
By assisting fellows in identifying their strengths and weaknesses, faculty advisors can help to ensure that fellows make informed long-term decisions regarding their area of practice based on their personal abilities and desires.
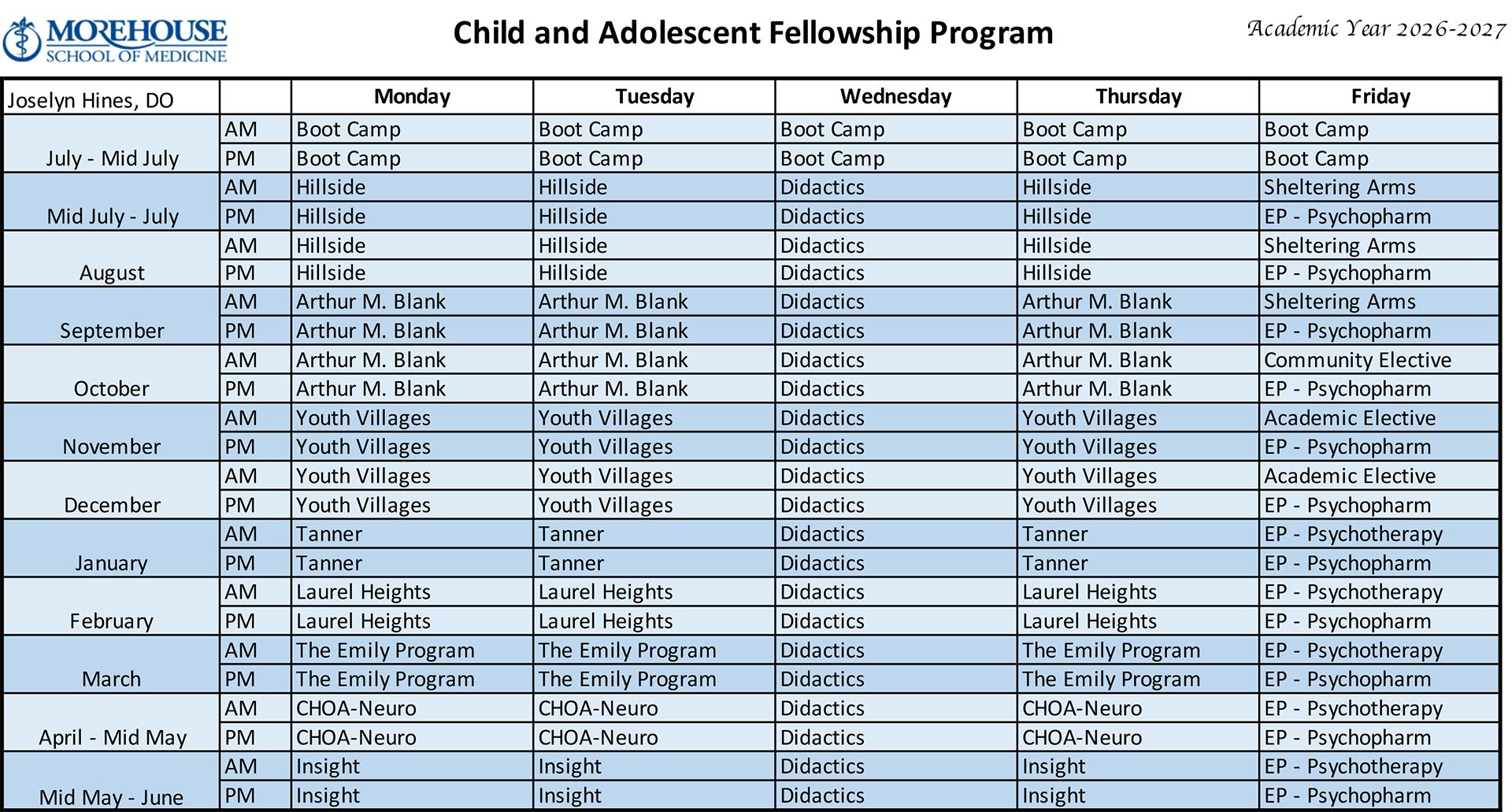
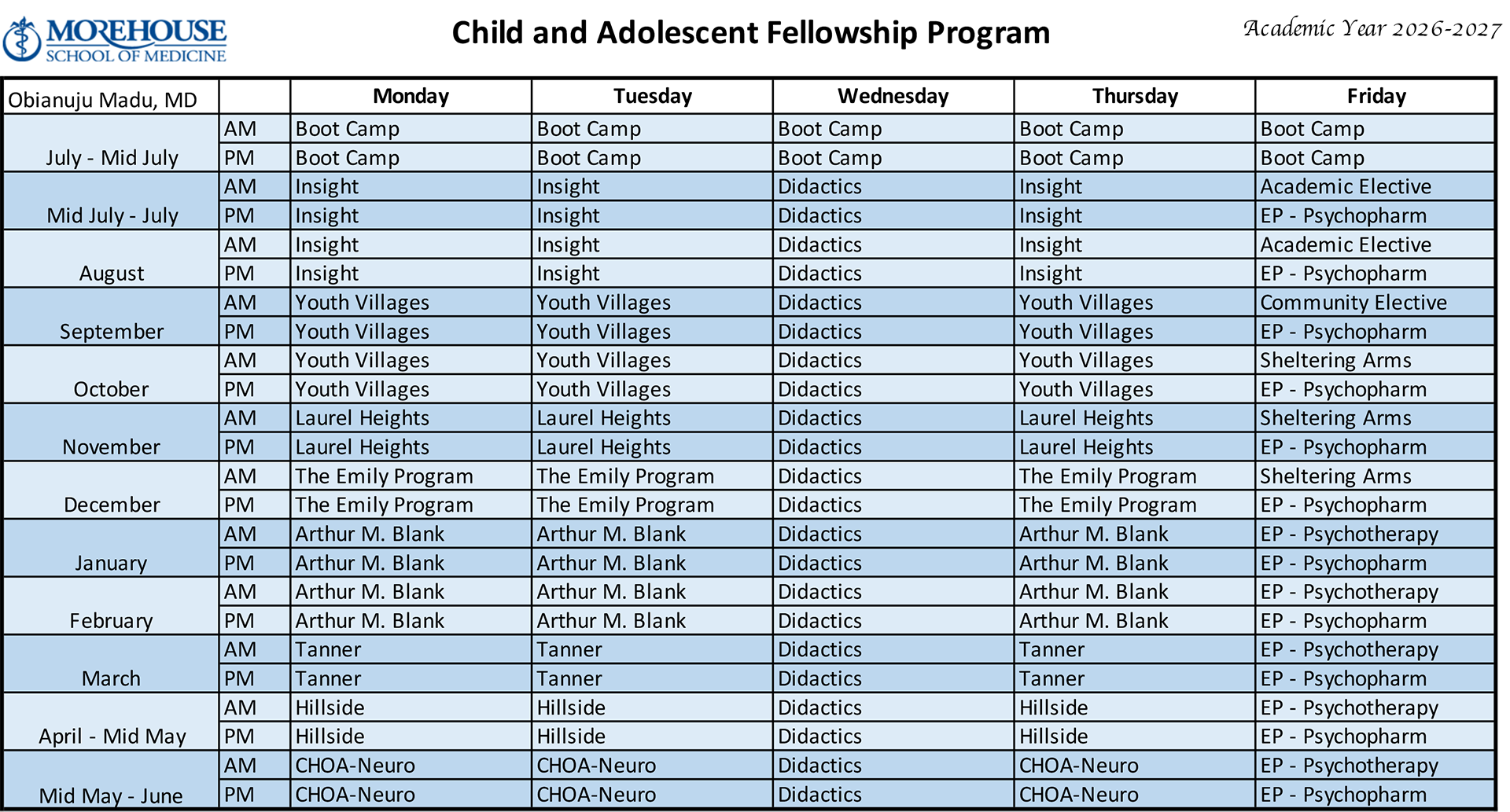
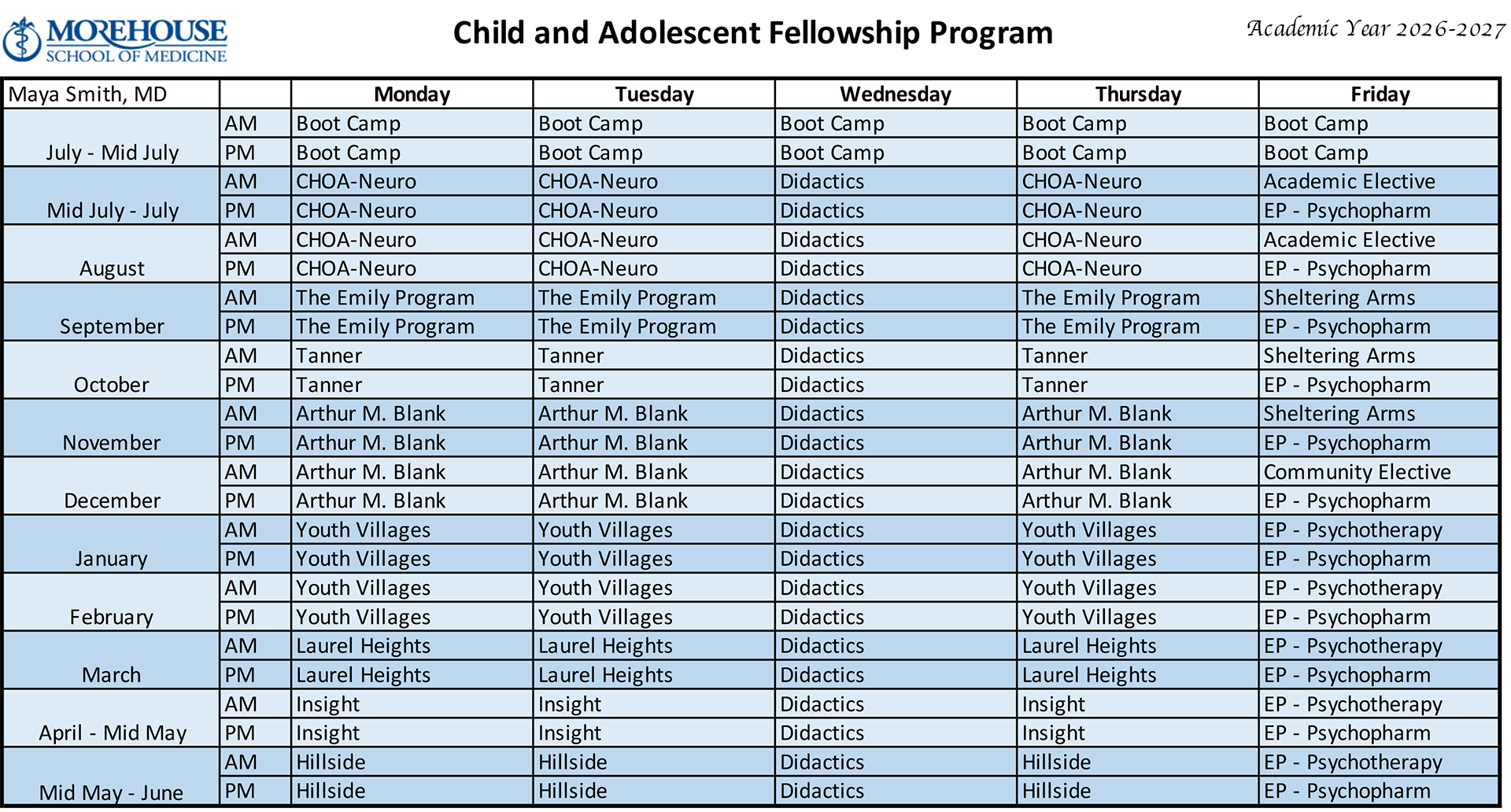
CAP Fellowship Master Clinical Schedules
Learning Activities
Courses
At a minimum, each fellow is expected to attend 70% of the regularly scheduled didactic sessions.
Each course carries an expectation that fellows prepare for class and then actively participate in the discussions. Syllabi for courses are housed in MedHub and OneDrive. The most up-to-date list of topics and readings is available on OneDrive.
Combined Class Courses
- Development and Psychopathology—Course Director, Dr. Kamille Williams
- Treatment Interventions—Course Director, Dr. Jenika Hardeman and Dr. LeRoy Reese
- Special Topics—Course Director, Dr. Kamille Williams and Certain Adjunct Faculty
- Bootcamp—Course Directors, Dr. Danae Evans and Dr. Kamille Williams
- Neuroscience and PRITE Review—Course Director, Dr. Kamille Williams and CAP Faculty
- CAP Process Group—Supervisor, Dr. Marietta Collins
- Fundamentals of Psychotherapy—Course Directors, Dr. Jenika Hardeman and Dr. LeRoy Reese
- Fundamentals of Treatment Interventions—Course Directors, Dr. Jenika Hardeman and Dr. LeRoy Reese
Biennial Combined Courses
- Black Child Psychiatry—Course Director, Dr. Sarah Y. Vinson
- Life of Children—Course Director, Dr. Sarah Y. Vinson
- Positive Psychiatry—Course Director, Dr. Sarah Y. Vinson
Second Year Courses
- Transition to Practice/Community and Consult—Course Director, Dr. Kamille Williams
Clinical Case Conference
Clinical Case Conferences are held the third Wednesday of every other month at 12 noon, virtually. These conferences include a review of topics and cases in child and adolescent psychiatry. The Clinical Case Conference is organized by and led by a fellow. The Fellow should reach out to the assigned faculty discussants in the syllabi two weeks in advance with the draft of their case conference and any supporting materials. Attendance at Clinical Case Conference is mandatory for fellows and there is an open invitation for any faculty member to attend.
Journal Club
Journal Club meetings are held on the first Wednesday of every other month at 12 noon, in person. Generally, two or three recent and/or landmark journal articles are discussed by both faculty and fellows. Fellows are taught how to critically appraise and evaluate the medical literature. The Journal Club is organized and led by a fellow. The fellow should reach out to the assigned faculty discussants in the syllabi two weeks in advance with the copy of the selected journal articles. Attendance at journal club is mandatory for fellows and there is an open invitation for any faculty member to attend.
Evaluations of Fellows
Multi-source evaluative feedback on performance and progress in the training program is provided to the fellows throughout their training.
Supervising Attendings and/or site directors, course directors, the fellowship program leadership, psychotherapy supervisors, and advisors all provide feedback via MedHub. Additionally, fellows are provided links to share with members of the multidisciplinary care team, patients, peers, and students for 360-degree evaluations. Fellows are also expected to perform self-evaluations. Twice a year, each fellow receives semi-annual evaluations by the program leadership. These evaluations are intended as a review of the overall progress of the fellow, to discuss any problems or concerns, and to identify goals for the upcoming year.
Midway through each rotation, the supervising Attending should meet with each fellow to discuss their mid-rotation evaluation, document their progress, and provide feedback on the fellow’s strengths and weaknesses. If this meeting is not initiated by the Attending, it should be initiated by the fellow. At the end of each rotation, the site supervisor and/or Attending completes a written evaluation on the performance of the fellow. The supervising Attending also meets with the fellow for end-of-rotation feedback. The faculty member evaluates the fellow on each of the six (6) core competencies established by the ACGME that are relevant for a given site:
- Professionalism
- Patient Care and Procedural Skills
- Medical knowledge
- Practice-Based Learning and Improvement
- Interpersonal and Communication Skills
- Systems-Based Practice
Evaluations by Fellows
Fellows must complete a formal evaluation via MedHub for each of their learning activities and rotations. They are also asked to provide feedback in monthly meetings with the program director and/or the associate program director.
Child PRITE Exam
One of the most valuable contributions of the American College of Psychiatrists (ACP) to psychiatric education is the annual Child Psychiatry Resident-In-Training Examination (PRITE®). The ACP designed the CHILD PRITE as an educational resource for psychiatric fellows and training programs. Each section of the exam focuses on a particular component of psychiatry, offering references to support and explain correct answers.
CHILD PRITE results provide helpful information for both fellows and training directors as well as for the residency program. Fellows receive a detailed computer analysis of their test performance in comparison with other fellows at a similar level of training. Training directors receive results for their individual fellows as well as statistical summary data comparing their training program with other groups of participants. Fellowship programs use CHILD PRITE as one factor, among many, for assessing the competency of fellows. This information assists training directors in adjusting their programs to make them more effective.
CHILD PRITE takes place in December. Nearly all psychiatry fellows in the United States, and many in Canada, take the exam both years of their fellowship training. At the MSM fellowship, fellows also take two PRITE-style self-assessment exams over the course of the academic year.
Scholarly Activity and PS/QI Project
Fellows are required to complete a scholarly project/presentation entitled Senior Talk, and to participate in a PS/QI project prior to graduation. Potential scholarly activities must be approved by the program director or the associate program director, and include, but are not limited to, following:
- Poster or oral presentation at a local, regional, or national conference
- Service on a national professional board
- Published letters to the editor
- Published case reports (all authors) and published research manuscripts (all authors)
- Partial or complete book chapters
Submitted manuscripts or posters which have not been accepted will be judged on a case-bycase basis.
Conferences and Presentations
Fellows may be selected to participate in conferences throughout the country. The Fellowship Program and the Department of Psychiatry work in collaboration to sponsor fellows for these important events with the following guidelines:
- Fellows must be in good standing, not on probation, and not have issues related to professionalism.
- An annual professional development stipend is provided for the fellow to use for conference travel and participation for the annual American Academy of Child and Adolescent Psychiatry. The amount of the sponsorship is based on availability of funds. This event is a required professional activity for Fellows and Faculty.
- Notification of invitation to present must be submitted to the program at least 60 days in advance, whenever possible.
- Time away for conferences is awarded based on rotation and number of administrative days available and is awarded at the discretion of the program director. Number of days off for job and fellowship interviews will also be taken into account.
- Preference is given when fellows are presenting or serving on a national committee that is meeting at the conference.
The subject matter of the research or presentation is determined by the fellow in consultation with their faculty advisor or research mentor. Fellows must provide the Fellowship Program Office with documentation of their abstract acceptance. All abstracts prepared by fellows for submission and presentation at scientific meetings should have a designated faculty/mentor reviewer. Fellows are responsible for obtaining faculty/mentor review and signature on the abstract submission forms. With the help of their faculty mentor, fellows should determine at the onset of proposed research whether the research activity planned requires MSM IRB review and approval.
Lead time for requested departmental support/reimbursement is critical. As soon as the fellow is notified of an acceptance for a presentation, the fellow MUST inform the fellowship program. At least two (2) months lead time is required for reimbursement. In the case of requests submitted less than two (2) weeks prior to the event, the fellow will be responsible to cover the initial cost and may not be reimbursed at the full cost of the travel expenses, with partial or complete reimbursement determined as funds allow.
MedHub and OneDrive
All official documents related to the fellowship can be accessed through MedHub and/or OneDrive. MedHub contains the official records for fellows: evaluations, time off requests, moonlighting permission requests, schedules, and the fellows’ portfolios. Schedules and syllabi housed there are updated at regular intervals by the program staff. The OneDrive folder is a more accessible, nimble online repository and will always include the most up-to-date syllabi, readings, and schedules. Additionally, it includes helpful information, such as faculty descriptions. Scholarly activity work product is stored here as well. Final projects are only entered into MedHub.
Web-Based Resources
To access books, full articles, and the other resources in the online library, no sign on is necessary when logging in on campus. However, when accessing the library resources off campus, sign on is required with the login name and password used to check webmail.
Among many other things, the MSM Online Library site provides access to:
- The Psychiatry Online Database
- PubMed and some full articles
- Ovid and some full articles. You may need to have this site open when you are trying to download articles from PubMed.
- UpToDate; this site is available only from on campus.
https://acgme.org/Portals/0/PDFs/ab_ACGMEglossary.pdf?ver=2018-05-14-095135-583
https://www.acgme.org/globalassets/pdfs/milestones/childandadolescentpsychiatrymilestones2.0.pdf
The term resident in this document refers to both specialty residents and subspecialty fellows. Common Program Requirements noted in each set of specialty and subspecialty requirements uses the terms resident and fellow interchangeably.
IV.B.1.a) Professionalism
Fellows must demonstrate a commitment to professionalism and an adherence to ethical principles.
IV.B.1.b) Patient Care and Procedural Skills
Background and Intent: Quality patient care is safe, effective, timely, efficient,
patientcentered, equitable, and designed to improve population health, while reducing
per capita costs. (See the Institute of Medicine [IOM]’s Crossing the Quality Chasm:
A New Health System for the 21st Century, 2001 and Berwick D, Nolan T, Whittington
J. The Triple Aim: care, cost, and quality. Health Affairs. 2008; 27(3):759-769.).
In addition, there should be a focus on improving the clinician’s well-being as a
means to improve patient care and reduce burnout among residents, fellows, and practicing
physicians.
These organizing principles inform the Common Program Requirements across all Competency
domains. Specific content is determined by the Review Committees with input from the
appropriate professional societies, certifying boards, and the community.
IV.B.1.b).(1) Fellows must be able to provide patient care that is compassionate, appropriate, and effective for the treatment of health problems and the promotion of health. (Core)
- IV.B.1.b).(1).(a) Fellows must demonstrate competence in:
- IV.B.1.b).(1).(a).(i) evaluation and treatment of patients representing the full spectrum of psychiatric illnesses in children and adolescents, including developmental and substance use disorders;(Core)
- IV.B.1.b).(1).(a).(ii) treatment of children and adolescents for the development of conceptual understanding and beginning clinical skills in major treatment modalities, including brief and long-term individual therapy, family therapy, group therapy, crisis intervention, supportive therapy, psychodynamic psychotherapy, cognitive-behavioral therapy, and pharmacotherapy;(Core)
- IV.B.1.b).(1).(a).(iii) evaluation and treatment of patients from diverse cultural backgrounds and varied socioeconomic levels; and,(Core)
- IV.B.1.b).(1).(a).(iv) performance and documentation of an adequate individual and family history; mental status; physical and neurological examinations when appropriate; supplementary medical and psychological data, and integration of these data into a formulation; differential diagnosis; and a comprehensive treatment plan. (Core)
IV.B.1.b).(2) Fellows must be able to perform all medical, diagnostic, and surgical procedures considered essential for the area of practice.(Core)
IV.B.1.c) Medical Knowledge
Fellows must demonstrate knowledge of established and evolving biomedical, clinical, epidemiological and social behavioral sciences, as well as the application of this knowledge to patient care.(Core)
IV.B.1.c).(1) Fellows must demonstrate competence in their knowledge of:
- IV.B.1.c).(1).(a) basic neurobiological, psychological, and clinical sciences relevant to psychiatry and the application of developmental, psychological, and sociocultural theories relevant to the understanding of psychopathology;(Core)
- IV.B.1.c).(1).(b) the full range of psychopathology in children and adolescents, including the etiology, epidemiology, diagnosis, treatment, and prevention ofmajor psychiatric conditions that affect children and adolescents;(Core)
- IV.B.1.c).(1).(c) recognition and management of domestic and community violence, including physical and sexual abuse, as well as neglect, as it affects children and adolescents;(Core)
- IV.B.1.c).(1).(d) diversity and cultural issues pertinent to children, adolescents, and their families; and,(Core)
- IV.B.1.c).(1).(e) the appropriate uses and limitations of psychological tests.(Core)
IV.B.1.d) Practice-based Learning and Improvement
Fellows must demonstrate the ability to investigate and evaluate their care of patients, to appraise and assimilate scientific evidence, and to continuously improve patient care based on constant self-evaluation and lifelong learning. (Core)
Background and Intent: Practice-based learning and improvement is one of the defining characteristics of being a physician. It is the ability to investigate and evaluate the care of patients, to appraise and assimilate scientific evidence, and to continuously improve patient care based on constant self-evaluation and lifelong learning.
The intention of this Competency is to help a fellow refine the habits of mind required to continuously pursue quality improvement, well past the completion of fellowship.
IV.B.1.e) Interpersonal and Communication Skills
Fellows must demonstrate interpersonal and communication skills that result in the effective exchange of information and collaboration with patients, their families, and health professionals. (Core)
IV.B.1.f) Systems-based Practice
Fellows must demonstrate an awareness of and responsiveness to the larger context and system of health care, including the social determinants of health, as well as the ability to call effectively on other resources to provide optimal health care. (Core)
Educational Program Requirements
Per ACGME Common Program Requirements Section IV., accredited programs are expected to define their specific program aims consistent with the overall mission of their Sponsoring Institution, the needs of the community they serve and that their graduates will serve, and the distinctive capabilities of physicians it intends to graduate.
IV.A. All MSM GME programs’ curriculum must contain the following educational components:
- A set of program aims consistent with the Sponsoring Institution’s mission, the needs of the community it serves, and the desired distinctive capabilities of its graduates.
- a. The program’s aims must be made available to program applicants, residents/fellows, and faculty members.
- Competency-based goals and objectives for each educational experience designed to promote progress on a trajectory to autonomous practice.
- a. These must be distributed, reviewed, and available to residents/fellows and faculty members.
- Delineation of resident responsibilities for patient care, progressive responsibility for patient management, and graded supervision.
- A broad range of structured didactic activities.
- a. Residents/fellows must be provided with protected time to participate in core didactic activities.
- Advancement of residents/fellows’ knowledge of ethical principles foundational to medical professionalism.
- Advancement in the residents/fellows’ knowledge of the basic principles of scientific inquiry, including how resident is designed, conducted, evaluated, explained to patients, and applied to patient care.
IV.B. ACGME Competencies – referenced and provided in detail above.
IV.C. Curriculum Organization and Resident Experiences – MSM GME programs must:
- Ensure that the program curriculum is structured to optimize resident educational experiences, the length of these experiences, and supervisory continuity.
- Provide instruction and experience in pain management, if applicable, for the specialty, including recognition of the signs of addiction.
- Resident/Fellow Scholarly Activity
- a. Residents and fellows must participate in scholarship activity.
The GME DIO and GMEC will provide oversight of programs’ compliance with required educational components during the annual institutional and program review process and procedures.
All MSM GME programs are required to:
- Track and document scholarly activity data annually for residents, fellows, and all faculty involved in teaching/advising/supervising, including both core and non-core faculty, as part of the Annual Program Evaluation (APE) process.
- Document and implement program-level scholarly requirements and guidelines that are distributed and reviewed with the residents, fellows, and faculty members on an annual basis.
Child and Adolescent Psychiatry Fellow Position Summaries
Title: CAP Fellow, First-Year, PGY-4 or PGY-5
Reports to: Program Director
First year fellows are expected to build upon the knowledge and skills gained during their Psychiatry General Residency training. First year fellows are under the supervision of senior fellows and Attendings. However, they are also expected to have enough prior medical experience and knowledge to supervise residents, interns, and medical students in psychiatry with Attending oversight. First year fellows will be expected to focus on gaining knowledge specific to the field of Child and Adolescent Psychiatry.
Title: CAP Fellow, Second Year, PGY-5 or PGY-6
Reports to: Program Director, Department of Psychiatry Faculty
Second year fellows are expected to focus on becoming experts in the clinical evaluation and treatment of children and adolescents with psychiatric disorders and should be able to practice evidence-based medicine for the full spectrum of child and adolescent mental illness. Additionally, they are expected to be able to apply their clinical and developmental knowledge to non-clinical settings in order to further their consultation and advocacy for education and collaboration in interdisciplinary settings.
By the end of their second year, fellows should be deemed capable of practicing independently in the field of child and adolescent psychiatry in a competent and safe manner. Second year fellows should fully meet all six (6) of the ACGME general core competencies. With faculty support, second year fellows should be able to submit the results of their research or community outreach project as an abstract to the appropriate forum, and will be encouraged to submit full-length manuscripts for publication in clinical and/or scientific journals and/or for presentation at national or state professional meetings.
Goals, Objectives, Key Personnel, and Site Information by Rotation
First Year
Child and Adolescent Academic Elective
Child and Adolescent Community Elective
Children's Healthcare of Atlanta, Inc. (CHOA)
The Emily Program
Hillside Atlanta
The Insight Program
Laurel Heights Hospital
Morehouse Health Care (MHC) Psychopharmacology
Morehouse Health Care (MHC) Psychotherapy
Children's Physician Practice Group Neurology Practice
Sheltering Arms
Willowbrooke Tanner
Youth Villages
Second Year
AUCC Student Health and Wellness
Barton Child Law and Policy Center at Emory University School of Law
Child and Adolescent Fellowship Patient Safety Quality Improvement
Children’s Healthcare of Atlanta Autism
East Point Psychotherapy
Familes First
Georgia Department of Juvenile Justice
Georgia LEND
Grady Infectious Disease Program Clinic
Medcura Health Center
Medcura School Based Health Center
Policies, Procedures, Processes, and Program Template
Child and Adolescent Fellowship Program Policies and Procedures 2026-2027
The Child and Adolescent Fellowship Program follows and complies with all policies, procedures, and processes of Morehouse School of Medicine MSM Human Resources and Graduate Medical Education.
All residents are responsible for reviewing and adhering to policies, procedures, and processe of the MSM and affiliate training sites.
The Graduate Medical Education Policy Manual can be found here.
Fellow Concern, Complaint, and Due Process Policy
I. PURPOSE:
I.1. The Child and Adolescent Psychiatry Fellowship Program follows all MSM and Graduate Medical Education (GME) policies for resident due process, concerns, and complaints available in the GME Policy Manual on the MSM website.
I.2. Refer to the online version of the MSM GME Policy Manual for detailed information regarding the Adverse Academic Decisions and Due Process policy.
II. RESIDENT CONCERN AND COMPLAINT PROCESS:
To ensure that residents are able to raise concerns, complaints, and provide feedback without intimidation or retalia-tion, and in the confidential manner as appropriate, the following options and resources are available and communi-cated to residents and faculty annually.
II.1. Step One
Discuss the concern or complaint with your chief resident, clinical service director, program manager, associate program director and/or program director as appropriate.
II.2. Step Two
If the concern or complaint involves the program director and/or cannot be addressed in Step One, residents have the option of discussing issues with the Department Chair, Dr. Nicole Cotton (cotton@msm.edu, (404) 756-1440) or chief of service of a specific hospital as appropriate.
II.3. Step Three
If you are not able to resolve your concern or complaint within your program, the following resources are available:
- II.3.1. For issues involving program concerns, training matters, or work environment, residents can contact the GME Executive Director, Susan Ratliff (sratliff@msm.edu, (470) 670-6962).
- II.3.2. For problems involving interpersonal issues, the Resident Association president or president elect may be a comfortable option to discuss confidential informal issues apart and separate from the Psychiatry Department.
- II.3.3. Residents can provide anonymous feedback/concerns/complaints to any department at MSM by completing the online form—GME Feedback. Comments are anonymous and cannot be traced back to individuals.
- II.3.4. Personal follow-up regarding how feedback/concerns/complaints have been addressed by departments and/ or GME will be provided only if residents elect to include their name and contact information in the comments field.
- II.3.5. MSM Compliance Hotline, 1-888-756-1364, is an anonymous and confidential mechanism for reporting un-ethical, noncompliant, and/or illegal activity. Call the Compliance Hotline to report any concern that could threaten or create a loss to the MSM community including:
- Harassment—sexual, racial, disability, religious, retaliation
- Environment Health and Safety—biological, laboratory, radiation, laser, occupational, chemical and waste management safety issues
- Other misuse of resources, time, or property assets; accounting, audit and internal control matters; falsification of records; theft, bribes, and kickbacks
Clinical Experience and Education Policy
I. PURPOSE:
I.1. Duty hours are defined as all clinical and academic activities related to the program, including inpatient and out-patient patient care assignments, administrative duties, call, scheduled activities such as conferences and moonlighting.
I.2. Duty hours do not include reading and preparation time spent away from the duty site.
I.3. Residents must adhere to all duty hour restrictions and requirements as outlined below:
- I.3.1. Duty hours must be limited to 80 hours/week, averaged over a four-week period.
- I.3.2. –Residents must have one (1) day in seven (7) free from all educational and clinical responsibilities, averaged over a four (4) week period.
- I.3.3. Residents should have 10 hours, must have eight (8) hours, free between all daily duty periods and call as-signments.
- I.3.4. In-house call must occur no more frequently than every fourth night for psychiatry rotations (no more fre-quently than every third night for medicine rotations), averaged over a four (4) week period.
- I.3.5. Continuous on-site duty must not exceed 24 consecutive hours. Residents may remain on duty for up to four (4) additional hours to maintain continuity of medical care as needed.
- I.3.6. No new patients may be accepted after 24 hours of continuous duty.
- I.3.7. Moonlighting is permitted for PGY-4 residents in good standing, with an independent medical license, and proper malpractice coverage. Residents wishing to moonlight must obtain written permission from the pro-gram director. See Moonlighting Policy for additional details. Moonlighting must not interfere with the ability of the resident to achieve the goals/objectives of the educational program nor interfere with duty hours. Internal moonlighting is considered part of the duty hour limitations.
- I.3.8. Residents must log duty hours daily into MedHub. Failure to log for five (5) days out of seven (7) will result in an e-mail notification of non-compliance to the program director and manager. Logging requirements include:
- I.3.8.1. Logging should be consistent with no gaps (for example, for lunch or travel).
- I.3.8.2. Conferences should be logged consistently as other duties with no gaps in between.
- I.3.8.3. Log “Call” duty type for in house call.
- I.3.8.4. For back-up call assignments, if the resident has to go into the hospital, use “Back Up-Called In” duty type. Back-up residents do NOT log if they do not go into the hospital.
- I.3.8.5. If your 24-hour shift is extended duty to post call transitions of patient care or mandatory confer-ences, avoid a violation by logging the following two duty types (1) post call and (2) conferences for the hours that extend beyond the 24 hour period.
- I.3.8.6. Log appropriate duty types for moonlighting, vacation, holiday/day off, or sick days.
- I.3.8.7. Each resident must enter written Justification or Cause in the event of a violation. Justifications apply to violations of 24+ or short break rule. Causes apply to any violation. Make sure to submit to the program director
II. PROTOCOL FOR EPISODES WHEN RESIDENTS REMAIN ON DUTY BEYOND SCHEDULED HOURS:
II.1. In unusual circumstances, residents, on their own initiative, may remain beyond their scheduled period of duty to continue to provide care to a single patient.
II.2. Justifications for such extensions of duty are limited to reasons of required continuity for a severely ill or unstable patient, academic importance of the events transpiring, or humanistic attention to the needs of a patient or family. Under those circumstances, the resident must:
- II.2.1. Appropriately hand over the care of all other patients to the team responsible for their continuing care.
- II.2.2. Document the reasons in MedHub for remaining to care for the patient in question.
- II.2.3. The program director reviews each submission of additional service and tracks both individual resident and program-wide episodes of additional duty.
II.3. Failure to Comply
- II.3.1. In all cases the program director should be informed of the occurrence and nature of the situation in which the respite rule might have been an issue regarding duty hour standards compliance.
- II.3.2. All duty hour violations are monitored and recorded in MedHub. Violations are automatically reported to the program director, chair, and manager electronically.
II.4. For residents at the PGY-2 level and above, 2011 ACGME requirements include duty hours work limit of 24 con-tinuous hours on duty.
- II.4.1. Residents may stay beyond that period for four (4) additional hours in order to carry out an effective patient care transfer.
- II.4.2. Beyond a 24-hour period of duty in the hospital the resident must have at least 14 hours free from duty.
- II.4.3. If a resident is in the situation where she or he will be out of compliance with the policy, the resident is re-quired to document the reasons for remaining to care for the specific patient and submit the information into MedHub.
- II.4.4. This documentation will allow the program director and/or the program manager to discuss the resident’s schedule with the resident with the goal of preventing future occurrences. In the short term, however, duty hour restrictions should not serve as a reason to jeopardize patient safety.
- II.4.5. Repeated instances of non-compliance will be regarded as failure to adhere to accepted standards of profes-sionalism.
II.5. MedHub notifies the program director of duty hour violations automatically. The residents are then asked to submit a justification for the violation into MedHub. The program director notes if the justification is acceptable, the program director, chief resident(s), and resident meet to review the cause for the violation. The program di-rector and chief resident then work with the resident(s) and service administrator to resolve future duty hour violations.
II.6 Reference the MSM GME Policy Handbook for all eligibility, selection and appointment requirements and policies that include:
- Technical standards and essential functions for appointment and promotion
- Non-immigrant applicants to residency programs
Fatigue Management and Mitigation Policy
I. PURPOSE:
This policy is designed to increase awareness of the faculty and residents in recognizing the signs of fatigue and sleep deprivation, the negative effects of sleep deprivation and fatigue on their ability to provide safe and effective patient care, and to identify strategies to minimize the effects of fatigue.
II. DEFINITION:
II.1. Fatigue is defined as a feeling of weariness, tiredness, or lack of energy than can impair a physician’s judgment, attention, and reaction time.
II.2. Signs and symptoms of fatigue include, but are not limited to: moodiness, depression, irritability, apathy, impov-erished speech, flattened affect, impaired memory and confusion, difficulty focusing on tasks, sedentary nodding off during conferences or while driving, and repeatedly checking work. These harmful effects can lead to med-ical errors and compromise patient safety.
III. POLICY ON PROGRAM RESPONSIBILITIES:
III.1. The resident and faculty will be educated on the hazards of sleep deprivation and fatigue in the workplace and in their personal lives during GME and Departmental Orientations annually, Semi-Annual Departmental Patient Safety Didactics, and through the completion of Professionalism and Patient Safety modules at least annually, faculty presentations during the Annual Program Review, and/or Faculty Meetings.
III.2. Residents will be provided with sound didactic and clinical education planned and balanced with concerns for pa-tient safety and resident wellbeing. The program will ensure that the learning objectives of the program are not compromised by excessive reliance on residents to fulfill service obligations. Didactic and clinical education must have priority in the allotment of resident’s time and energy.
III.3. Faculty will assess if residents asleep-deprivedved and make appropriate recommendations for the resident to cor-rect this problem.
III.4. Faculty members are to assist in enforcing the limitations of the role of a resident under the duty hour mandates.
IV. POLICY ON RESIDENT RESPONSIBILITIES:
IV.1. The resident is expected to:
- IV.1.1. A dopt habits that will provide him or her with adequate sleep in order to perform the daily activities required by the program.
- IV.1.2. Adhere strictly to Duty Hour limitations.
- IV.1.3. Discuss time and stress management with their faculty advisors at least monthly.
IV.2. In the event that the resident is at the end of a work period and is too sleepy to drive home, he or she is encour-aged to use another form of transportation or nap prior to leaving the training site. The program will reimburse the resident as indicated when alternative transportation methods are utilized.
- IV.2.1. The resident should contact the chief resident, program director, or associate program director for assistance if neither of the aforementioned options is feasible.
- IV.2.2. MSM provides access to appropriate and confidential counseling and medical and psychological support ser-vices. Residents are encouraged to utilize EAP or their own physician and the Office of Disability Services when indicated.
ACGME Program Requirements for Graduate Medical Education in Child and Adolescent Psychiatry